Overview
Botulinum toxin type A (BTX-A) is among the most widely administered aesthetic treatments globally, yet the gap between technically performing an injection and understanding the clinical rationale behind every decision remains significant. This module establishes a rigorous decision-making framework built around five clinical principles — the 5 D’s — and grounds those principles in a thorough understanding of facial muscle anatomy and the relationships between muscle groups.
The module is designed for registered injectors with foundational anatomy knowledge. If you have not completed Module 03.01 — Facial Muscle Anatomy, completing that first is strongly recommended.
History & Mechanism of Action
A Brief History
Botulinum toxin was first identified in the context of food poisoning from Clostridium botulinum in the 19th century. Its therapeutic potential emerged when ophthalmologist Dr Alan Scott began investigating it as a treatment for strabismus in the 1970s, recognising that precise, localised muscle weakening could be clinically useful. The first FDA approval for medical use followed in 1989. Cosmetic approval for glabellar lines in the United States came in 2002, and Australian TGA approval for cosmetic indications followed. Today, BTX-A is one of the most studied biological medicines in clinical use, with an established safety profile across decades of therapeutic and aesthetic application.
Mechanism of Action
BTX-A exerts its effect at the neuromuscular junction. Under normal physiology, a nerve impulse triggers the release of acetylcholine (ACh) from vesicles in the motor nerve terminal via the SNARE protein complex — a group of proteins (SNAP-25, synaptobrevin, syntaxin) that facilitate vesicle docking and fusion with the nerve membrane.
BTX-A cleaves SNAP-25, a critical component of the SNARE complex, preventing vesicle fusion and blocking ACh release. Without ACh stimulation, the muscle cannot contract. The result is a temporary, localised, chemically-induced denervation of the targeted muscle.
The clinical onset of muscle relaxation typically occurs at 3–5 days post-injection, with full effect at 10–14 days. This informs the timing of clinical review appointments.
The 5 D’s: A Clinical Decision Framework
The following framework provides a structured approach to every neuromodulator treatment. Applied consistently, the 5 D’s reduce variability, support clinical reasoning, and build a defensible treatment rationale.
1 — Diagnosis
Diagnosis in the context of neuromodulator treatment means a clinical assessment of the muscle or muscle group being considered for treatment. This is not a passive observation — it is a structured evaluation that should occur before every treatment session, not assumed from prior visits.
Dynamic assessment is paramount. Ask the patient to produce the expression associated with the target concern — frowning, raising brows, smiling, clenching. Observe which muscles activate, their relative strength, and whether any compensatory patterns are present. A patient who lifts their brows substantially to compensate for early brow ptosis has a very different clinical picture from one with a genuinely overactive frontalis.
Static assessment follows — evaluating lines at rest reveals where dermal damage has already occurred from repeated muscle contraction. Static lines at rest do not resolve fully with neuromodulator treatment alone and require management expectation-setting with the patient.
Grade 1 — Minimal activity, fine surface lines only
Grade 2 — Moderate activity, visible lines on expression
Grade 3 — Strong activity, visible lines at rest in some positions
Grade 4 — Dominant activity, deep static lines at rest
Dose decisions should be informed by grade. A Grade 1 frontalis requires a materially different approach to a Grade 4.
Document your grading in the clinical record. This enables meaningful comparison at review and supports evidence-based dose adjustments over treatment cycles.
2 — Dose
Dosing in BTX-A treatment is not a fixed prescription — it is a clinical decision informed by muscle grade, treatment area, patient anatomy, prior treatment history, and desired outcome. Starting conservatively and adjusting at review is preferable to over-treating and managing an adverse outcome.
| Treatment Area | Muscle(s) | BTX-A Range | Points | Notes |
|---|---|---|---|---|
| Horizontal forehead lines | Frontalis Elevator | 10–20 units | 4–6 | Treat conservatively. Always assess brow position. Avoid inferior injection points below mid-pupil line. |
| Glabellar complex (“11s”) | Corrugator & Procerus Depressor | 20–30 units total | 5 | Standard 5-point technique. Corrugators bilateral (2 pts each), procerus central (1 pt). Treat simultaneously. |
| Lateral canthal lines (“crow’s feet”) | Orbicularis Oculi Sphincter | 8–20 units per side | 3–4 per side | Stay ≥1cm lateral to orbital rim. Inject superficially, subcutaneous plane. Treat bilaterally. |
| Brow shaping — medial depression | Corrugator (medial) Depressor | 4–8 units per side | 1–2 per side | Advanced technique for brow shaping. Requires precise anatomical knowledge of corrugator origin. |
| Downturned mouth corners | Depressor Anguli Oris Depressor | 2–5 units per side | 1 per side | Palpate the DAO carefully lateral to commissure. Avoid orbicularis oris — asymmetric lip droop risk. |
| Chin dimpling / peau d’orange | Mentalis Depressor | 4–10 units total | 2 | Paired muscle bellies, central chin. Risk of chin ptosis with over-treatment. Frequently combined with DAO. |
| Vertical neck bands | Platysma Depressor | 20–60 units total | Variable per band | Nefertiti lift technique. Multiple points along each visible platysmal band. Advanced — reassess at 4 weeks. |
| Bunny lines | Nasalis Depressor | 4–8 units total | 2 | Commonly a compensatory response to glabellar treatment. Assess whether treating the cause addresses the effect. |
3 — Depth
Accurate depth of injection determines whether the product reaches the intended target. Injecting too superficially results in suboptimal muscle effect and increased risk of superficial spread to non-target structures. Injecting too deeply risks reaching unintended muscles or neurovascular structures.
Facial muscles sit at varying depths depending on their anatomical layer:
- Superficial muscles (frontalis, orbicularis oculi at lateral canthus, nasalis, platysma) lie immediately deep to the dermis and subcutaneous fat. A superficial to mid-depth injection reaches these muscles effectively.
- Deep muscles (corrugator supercilii, depressor anguli oris) lie beneath more superficial muscular layers. The corrugator in particular lies beneath the frontalis and orbicularis oculi — a superficial injection here deposits product in the wrong plane. Palpation of the muscle belly before injection is essential.
- Mentalis lies centrally in the chin, embedded between the skin and the mandibular periosteum. A mid-depth injection into the muscle belly is appropriate.
4 — Direction
Direction encompasses the angle of needle entry, the orientation of the bevel, and the intended trajectory to the target muscle. It is inseparable from depth — direction and depth together define the needle’s endpoint.
Entry point selection should consider the target muscle’s location, the overlying structures to avoid (vessels, nerves, glands), and the diffusion pattern of the product from the depot point. For example, when treating the corrugator, entering from a lateral approach and angling medially and superiorly helps avoid the supratrochlear vessels that run medially.
Fan techniques distribute product from a single entry point along a muscle belly, reducing the number of punctures for the patient while maintaining coverage. This is commonly applied to the platysma and orbicularis oculi.
5 — Distribution
Once injected, BTX-A diffuses outward from the depot in an approximately radial pattern. The radius of clinically significant diffusion from a single injection point is approximately 1–1.5 cm, though this is influenced by the volume injected, dilution used, and the specific tissue characteristics at the site.
Multiple injection points are used when a muscle belly extends beyond the diffusion radius of a single depot — the frontalis being the prime example, where 4–6 points are typically required to cover the full active muscle. Conversely, a small muscle like the procerus is adequately covered with a single central depot.
Extrusion volume directly influences diffusion spread. A larger volume deposited in a single location increases the radius of diffusion. This is relevant when seeking broad coverage with fewer injections, but must be balanced against the risk of unintended spread to adjacent structures (for example, the levator palpebrae superioris in the upper lid from a corrugator injection).
Treating Holistically: The Interconnected Muscle System
The most clinically significant shift in aesthetic neuromodulator practice over the past decade has been moving away from treating isolated areas toward understanding the face as a dynamic system of opposing forces. Elevators and depressors exist in a state of balance. Relaxing one without considering its antagonist creates predictable and avoidable complications.
↑ Elevators
- Frontalis (brow)
- Levator labii superioris
- Zygomaticus major & minor
- Levator anguli oris
- Risorius
↓ Depressors
- Corrugator supercilii
- Procerus
- Depressor anguli oris (DAO)
- Depressor labii inferioris
- Mentalis
- Platysma
Clinical Scenarios
Scenario A — Treating corrugators without addressing frontalis
When the corrugators and procerus are relaxed, the medial brow loses its primary depressor influence. If the frontalis is not concurrently treated or assessed, a compensatory lateral brow elevation (“Spock brow” or “Mephisto brow”) can result, as the mid-lateral frontalis fibres remain active while the medial fibres are not opposed. The solution is to address lateral frontalis fibres simultaneously with the glabellar complex.
Scenario B — Treating frontalis without considering brow position
The frontalis is the sole brow elevator. In a patient with early brow ptosis who is using frontalis overactivity to compensate and maintain brow height, aggressive frontalis treatment will worsen the ptosis. Always assess brow resting position and compensatory activity before treating. A patient with Grade 4 frontalis but true brow ptosis may benefit more from minimal frontalis treatment plus brow repositioning adjuncts than from a standard dose approach.
Scenario C — Treating DAO for downturned mouth without assessing the lower face system
The DAO pulls the oral commissure inferiorly. Its antagonist is the levator anguli oris (LAO), which elevates the corner. Relaxing the DAO in isolation is effective when LAO is of adequate strength — but if LAO is also weak or hypotonic, treating DAO produces only partial improvement. A more comprehensive lower face approach may involve also assessing the mentalis, depressor labii inferioris, and orbicularis oris. Treating the lower face as a balanced system rather than individual muscles produces more consistently satisfying outcomes.
Scenario D — Treating a concern versus treating the system
Sometimes the correct clinical decision is not to treat all interconnected muscles. A patient seeking softening of dynamic forehead lines without loss of expressivity may request conservative frontalis treatment only. A patient who has a specific functional concern (e.g., brow asymmetry driven by unilateral corrugator dominance) may benefit from targeted unilateral treatment rather than a whole-face approach. Clinical nuance requires being able to assess when a targeted, concern-specific treatment is more appropriate than a holistic one.
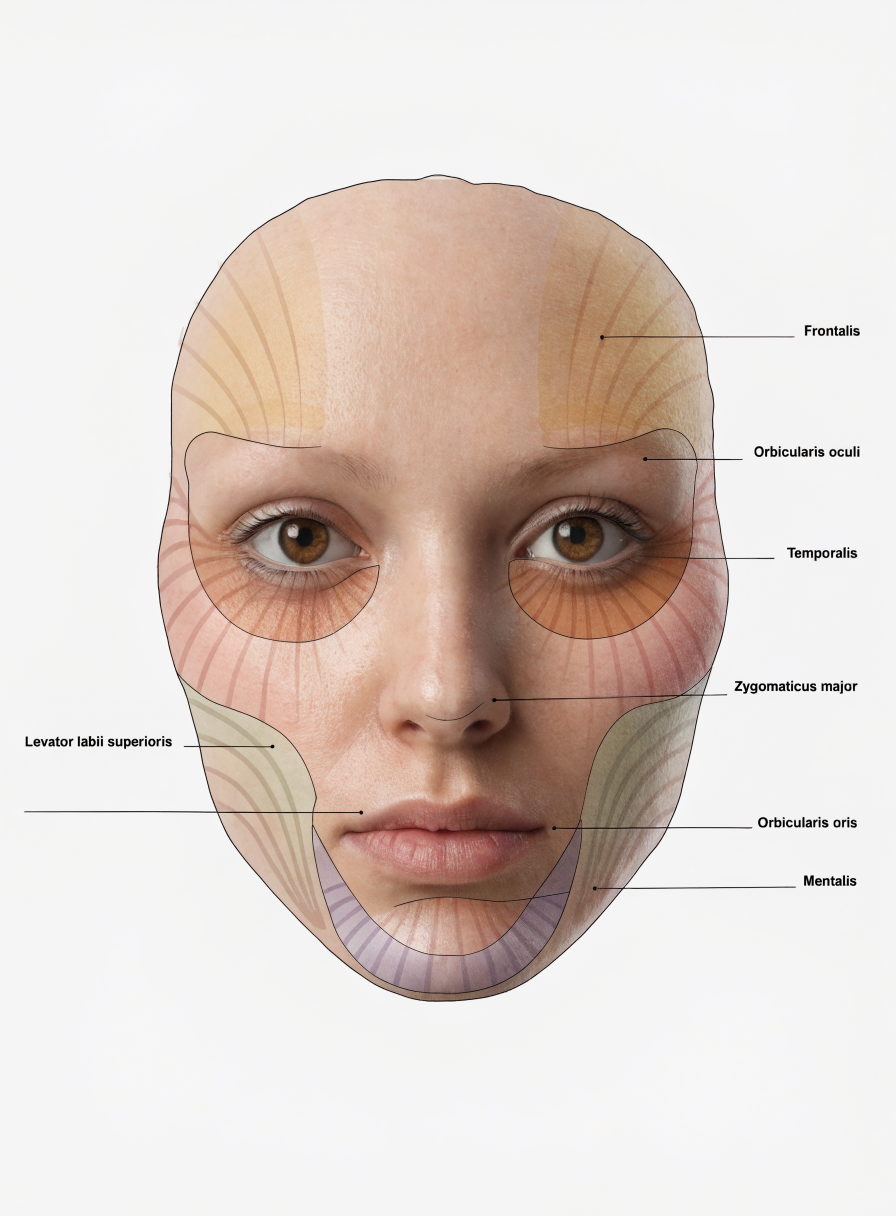
Interactive Facial Muscle Map
Select any muscle zone to view its clinical profile, recommended depth, dose range, and key interconnections. Use this as a reference tool when planning treatment — clicking a connected muscle highlights it on the diagram.
Learning Check
Five questions covering the core principles of this module. Select the best answer for each question then check your score.
Practitioner Feedback
Your input on clinical accuracy, content gaps, and level appropriateness shapes the final module. This form takes approximately 3–5 minutes.